 ,*,2), 薛贺波*, 杨刚*, 逄燕*, 房永超*, 李梦麒*, 齐轶鹏*, 史艺?
,*,2), 薛贺波*, 杨刚*, 逄燕*, 房永超*, 李梦麒*, 齐轶鹏*, 史艺?PIV EXPERIMENTAL STUDY ON THE HEMODYNAMICS OF AORTIC VALVE UNDER VARIED TILTED ANGLES 1)
Liu Zhaomiao,*,2), Xue Hebo*, Yang Gang*, Pang Yan*, Fang Yongchao*, Li Mengqi*, Qi Yipeng*, Shi Yi?通讯作者: 2) 刘赵淼,教授,主要研究方向:微尺度流体力学、血流动力学、流固耦合理论及工程应用. E-mail:lzm@bjut.edu.cn
收稿日期:2020-06-29接受日期:2020-08-7网络出版日期:2020-11-18
| 基金资助: |
Received:2020-06-29Accepted:2020-08-7Online:2020-11-18
作者简介 About authors

摘要
瓣叶血栓是主动脉瓣置换术后典型的继发性瓣膜疾病,血流动力学特征异常在其发展过程中至关重要.本文利用粒子图像测速 (particle image velocimetry,PIV) 系统,实验研究了主动脉瓣开口纵向轴线与升主动脉纵向轴线之间倾斜角度 ($\alpha =0^\circ$, $\alpha=5^\circ$,$\alpha =10^\circ$ 和 $\alpha =15^\circ$) 对速度、涡度和黏性剪应力分布等血流动力学特性的影响.研究结果表明:当 $\alpha =0^\circ$ 时,主动脉根部跨瓣血液流动为中心对称流动,而 $\alpha =5^\circ$,$\alpha=10^\circ$ 和 $\alpha =15^\circ$ 时跨瓣血液流动向升主动脉的左冠状动脉一侧倾斜.随着倾斜角度增大,跨瓣血液流动方向倾斜程度增加,血液流动冲击升主动脉壁,损伤内皮细胞导致血栓形成.主动脉瓣倾斜时主动脉窦血液流动速度增大,涡旋也更向主动脉窦底部运动,不利于血液从冠状动脉口流出向心肌供血.同时,主动脉根部的高涡度和高黏性剪应力区域也向升主动脉的左冠状动脉一侧倾斜,主动脉窦的高涡度区域位于主动脉窦底部、高黏性剪应力区域分布于主动脉窦壁面处.主动脉瓣存在倾斜角度时,涡度和黏性剪应力较大,特别是 $\alpha =10^\circ$ 和 $\alpha=15^\circ$,为血栓形成提供了有利环境.研究结果可为临床主动脉瓣置换术参数选择以及继发性瓣膜疾病的避免提供理论依据和技术参考.
关键词:
Abstract
Leaflet thrombosis is a typical secondary valvular disease after aortic valve replacement, and abnormal hemodynamic characteristics are crucial in its development. In this study, the effects of angle between the longitudinal axis of the aortic valve and that of the ascending aorta ($\alpha =0^\circ$, $\alpha =5^\circ$, $\alpha =10^\circ$ and $\alpha =15^\circ$) on the velocity, vorticity and viscous shear stress distribution are investigated using particle image velocimetry (PIV). It is of great significance to understand the hemodynamic mechanism of thrombosis after aortic valve replacement. The results show that the transvalvular flow in the aortic root is centrosymmetric flow when $\alpha =0^\circ$, while it tilts to the side of left coronary artery when $\alpha =5^\circ$, $\alpha =10^\circ$ and $\alpha =15^\circ$. The transvalvular flow tilts with the increasing of tilted angle and impacts on the wall of the ascending aorta, damaging the endothelial cells and causing thrombosis. In addition, the velocity within the aortic sinus increases and the vortex also moves toward the bottom of the aortic sinus with aortic valve tilted, which is unfavorable for the blood flowing from the coronary artery ostium to the myocardium for blood supply. Meanwhile, the high vorticity and high viscous shear stress area of the aortic root also tilts to the side of left coronary artery. And the high vorticity area of the aortic sinus is located at the bottom of the aortic sinus and the high viscous shear stress area is distributed at the wall of the aortic sinus. The vorticity and viscous shear stress are realy high when there is a mismatch between the ascending aorta longitudinal axis and that of the aortic valve, especially $\alpha =10^\circ$ and $\alpha =15^\circ$, providing a favorable environment for thrombosis. The results benefit to contribute theoretical bases and technical reference for the selection of clinical aortic valve replacement surgical parameters and that of the avoidance of secondary valvular disease.
Keywords:
PDF (31896KB)元数据多维度评价相关文章导出EndNote|Ris|Bibtex收藏本文
本文引用格式
刘赵淼, 薛贺波, 杨刚, 逄燕, 房永超, 李梦麒, 齐轶鹏, 史艺. 主动脉瓣倾斜角度血流动力学的 PIV 实验研究1). 力学学报[J], 2020, 52(6): 1811-1821 DOI:10.6052/0459-1879-20-229
Liu Zhaomiao, Xue Hebo, Yang Gang, Pang Yan, Fang Yongchao, Li Mengqi, Qi Yipeng, Shi Yi.
引言
主动脉瓣疾病是全世界发病率和致死率较高的典型心血管疾病之一,严重影响寿命和生活质量[1-3]. 外科主动脉瓣置换术和经导管主动脉瓣置换术是分别通过外科手术和介入导管技术,以人工生物瓣膜或机械瓣膜替换病变主动脉瓣的手术方式,是主动脉瓣疾病高危患者的有效治疗方案[4-6].据估计,全球有超过 1200 万人受到主动脉瓣疾病的影响,每年大约进行 30 万瓣膜置换术[7-8].尽管主动脉瓣置换术有效恢复瓣膜功能和改善血液流动状况,但由于个体化主动脉根部的影响,主动脉瓣的置换位置与生理位置存在错位,导致主动脉瓣血流动力学改变引发继发性瓣膜疾病,继而影响手术治疗效果[9-12].血流动力学因素在主动脉瓣置换术后继发性瓣膜疾病的发生中扮演至关重要的角色[13].主动脉瓣附近的粒子停留时间过长,易形成瓣叶溶血. 升主动脉中较高的剪应力,损伤血液中的血细胞.主动脉瓣瓣口的射流冲击主动脉壁面,损伤内皮细胞并逐渐形成血栓[14].
在主动脉瓣置换术主动脉瓣定位血流动力学研究中,其中主动脉瓣深度、旋转角度、倾斜角度是影响瓣膜附近血流动力学的重要因素,多位****围绕不同的主动脉瓣深度,利用粒子图像测速 (particle image velocimetry,PIV) 技术开展血流动力学研究,发现主动脉瓣深度显著影响主动脉窦的血液流动和主动脉根部的雷诺剪应力分布,结果表明主动脉瓣深度处于生理瓣环位置时流体动力学性能最优[15-17].
主动脉瓣在主动脉根部中的位置存在旋转角度和倾斜角度等定位误差时,也会改变主动脉瓣血流动力学行为,表现为血流速度、涡度和黏性剪应力等血流特性的异常,与细胞溶血和血栓形成等继发性瓣膜疾病密切相关[18-23].Bailey 等[24]从 0$^\circ$$\sim$105$^\circ$ 每间隔 15$^\circ$ 建立主动脉瓣模型,通过数值模拟研究旋转角度对瓣叶范式等效应力的影响,发现除了旋转角度为 30$^\circ$ 时,所有主动脉瓣模型的平均范式等效应力减小,最大范式等效应力在旋转角增大至 60$^\circ$ 后开始减小.表明最佳旋转角度为 0$^\circ$,最不可取的旋转角度是 30$^\circ$ 和 60$^\circ$.Hatoum 等[20]基于 CT 图像三维重构主动脉根部,利用 PIV 技术研究了主动脉瓣不倾斜、向主动脉窦倾斜和远离主动脉窦倾斜 3 种情况下主动脉窦中的血液流动停滞现象,发现两种倾斜情况下主动脉窦中血液流动速度、涡度和瓣叶附近剪应力降低,主动脉瓣远离主动脉窦倾斜时最不宜血液和粒子流出主动脉窦.尽管该研究对主动脉瓣不同倾斜情况时主动脉窦中的血流动力学进行了分析,但缺少对不同倾斜角度下的血流动力学研究.Morganti 等[12]基于 CT 图像重建主动脉瓣,建立有限元模型,研究了主动脉瓣倾斜角度对应力和有效开口面积的影响,结果表明主动脉瓣倾斜时应力增大、有效开口面积减小.但该研究仅分析了主动脉根部瓣叶附近三角区的应力,缺乏对主动脉根部中血液流动速度分布和黏性剪应力等血流动力学的分析.
目前,有关主动脉瓣置换术瓣膜定位误差的研究主要集中于不同主动脉瓣植入深度血流动力学,而对倾斜角度的关注相对较少且多为瓣叶应力分析,具体倾斜角度时瓣叶下游的血液流动和剪应力环境研究较为缺乏.本文基于医学影像数据三维重构真实主动脉根部,制备高度光滑、透明的实验模型,建立体外脉动循环模拟系统,利用 PIV 技术实验研究不同主动脉瓣倾斜角度对瓣叶下游的速度分布、涡度和黏性剪应力等血流动力学的影响,揭示主动脉瓣置换角度错位的血流动力学机理.
1 材料与方法
1.1 实验模型
选择一例共 228 张、层厚 0.5 mm 的正常人体心脏 CT 图像数据,进行主动脉根部模型建立[25-27]. 利用 Mimics 18.0 (Materialise, Leuven,Belgium) 进行分割,如图1(a) 所示,三维重构主动脉根部模型,如图1(b) 所示. 通过触觉式设计系统 Free Form (3D Systems, USA),对模型表面进行光滑处理,完成主动脉根部几何模型建立,模型包括升主动脉、主动脉窦和左心室流出道,如图1(c) 所示. 选择水溶性材料聚乙烯醇 (polyvinyl alcohol, PVA),利用 3D 打印技术打印主动脉根部 PVA 模型,以聚二甲基硅氧烷 (polydimethylsiloxane,PDMS) 浇筑主动脉根部,并水浴溶解 PVA 后得到高度光滑和透明的主动脉根部 PDMS 实验模型,如图1(d) 所示.图1
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图1主动脉根部模型建立
Fig. 1Establishment of the aortic root
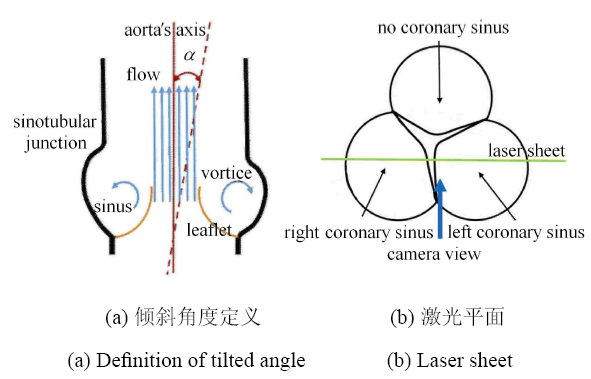
主动脉瓣为瓣环直径 25 mm 的美敦力 Hancock II T510 型生物主动脉瓣 (Medtronic, Minneapolis, USA). 倾斜角度 ($\alpha $) 是主动脉瓣开口纵向轴线与升主动脉纵向轴线之间的角度,如图2(a) 所示. 主动脉瓣存在倾斜时主动脉窦中血流特性改变,导致血液和粒子不易流出主动脉窦,但具体倾斜角度的血流动力学研究较为缺乏.根据主动脉 瓣置换术临床影像数据的倾斜角度范围[20, 28],本文研究主动脉瓣向左冠状动脉一侧 倾斜时,$\alpha=0^\circ$, $\alpha =5^\circ$, $\alpha =10^\circ$ 和 $\alpha =15^\circ$ 的血流动力学. 实验时,相机位置和经过主动脉瓣的激光平面如图2(b) 所示.
图2
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图2倾斜角度定义和激光平面
Fig. 2Definition of tilted angle and Laser sheet
1.2 实验装置
PIV 技术是一种非侵入式的全流场流动测量及显示技术,广泛应用于主动脉瓣的速度场和剪应力环境研究[15-17].PIV 系统主要由双脉冲 Nd:YAG 激光器 (Dantec Dynamics,Denmark;能量 20 mJ,波长 532 nm,脉冲时间 4 ns)、CCD 相机 (HiSense MKII, DantecDynamics)、同步控制器、片光元件、导光臂和计算机组成[29-35],如图3(a) 所示.双脉冲 Nd:YAG 激光器产生激光,经过导光臂、柱面镜和球面镜等片光元件引导后,激光在实验模型中心平面形成厚度约为 1 mm 的片光,激发均匀布撒于工作流体中的荧光粒子. 通过带有尼康镜头 (LaVision, Germany,Imager Pro;像素 1344 $\times$ 1024 Px) 的 CCD 相机记录单位时间内荧光粒子的两帧图像,利用 DynamicStudio (Dantec Dynamics, Denmark) 软件处理后获得目标流场.CCD 相机镜头上安装 570 nm 长波通滤光片阻止自然光进入 CCD 相机,同时使荧光粒子发出的光进入 CCD 相机.实验时两帧时间间隔设置为 250 $\mu $s,拍摄频率为 7 Hz.图3
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图3实验系统
Fig. 3Experimental system
体外脉动循环系统模拟左心室血液循环,由脉动式血液泵 (Harvard Apparatus,USA)、储液池、压力计、节流阀和顺应腔等组成[36],如图3(b) 所示. 脉动式血液泵用于模拟心脏功能,作为动力 源驱动循环系统工作.顺应腔和节流阀通过管路与升主动脉出口连接,用于调节升主动脉出口的平均压力.节流阀控制进入顺应腔的工作流体,压缩顺应腔中的可压缩空气,使升主动脉出口达到主动脉瓣最大张开幅度的平均压力.工作流体由脉动式血液泵从储液室中泵出进入主动脉根部,流经主动脉瓣后到达三通管,一路进入顺应腔,另一路经节流阀后回到储液池,形成循环.
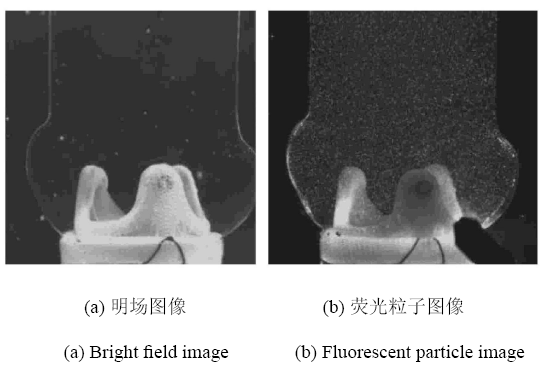
实验设置脉动式血液泵的心率为 70 Beats/min,每搏出量为 70 mL,收缩期/舒张期为 35%/ 65%.工作流体选 择体积比为 40%/ 60% 的丙三醇/去离子水混合溶液,其物理性质类似于血液,密度 $\rho=1100$ kg/m$^{3}$、常温 时黏度 $\mu\!=\!4.0$ mPa$\cdot$s,折射率 $(n\!=\!1.38)$ 与主动脉根部 PDMS 模型折射率相近 $(n=1.41)$[37].荧光粒子为直径 $1\sim 20 \mu $m 的 PMMA-Rhod- amine B 粒子 (Dantec Dynamics,Denmark),主动脉根部明场图像和荧光粒子图像如图4 所示.
图4
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图4主动脉根部实验图像
Fig. 4Experimental image of the aortic root
2 结果与讨论
2.1 倾斜角度对主动脉瓣下游速度分布的影响
主动脉瓣张开和关闭是一个复杂的流体力学机制,主要受主动脉根部血液流动和循环变 化调节[38].图5 为 $\alpha =0^\circ$ 时心动周期内主动脉根部血液流动的平均速度云图,展示了心动周期内主动脉根部的血液流动状况. 收缩早期,主动脉瓣瓣叶开始张开,瓣口处出现血液流动,如图5(a) 所示. 加速期,主动脉瓣瓣叶张开幅度增大,血液流过主动脉瓣时形成中心对称流动,并且向升主动脉进一步流动,如图5(b) 所示. 峰值期,主动脉瓣瓣叶完全打开,血液中心对称流动加剧,血液跨瓣流动达到最大速度 1.56 m/s,如图5(c) 所示. 收缩晚期,主动脉瓣开始关闭,主动脉瓣附近的血液流动现象与峰值期现象相似,但流动速度降低,如图5(d) 所示. 舒张早期,随着主动脉瓣的关闭,跨瓣流动逐渐消失,如图5(e) 所示. 舒张晚期,瓣膜完全关闭,主动脉瓣口血液流动现象停止,主动脉根部中血液速度趋近于零,如图5(f) 所示.图5
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图5$\alpha =0^\circ$ 时主动脉根部速度云图
Fig. 5Velocity contours of the aortic root at $\alpha =0^\circ$
主动脉根部是血液流过主动脉瓣后的重要运输和物质交换场所,其血流动力学在主动脉瓣功能和血液正常流向冠状动脉中扮演至关重要 的角色[39].不同主动脉瓣倾斜角度时,峰值期主动脉根部血液流动平均速度分布云图如图6 所示. 峰值期,主动脉瓣完全张开,血液充分跨瓣流向升主动脉. 当 $\alpha=0^\circ$ 时,跨瓣血液流动状态为中心对称射流,左冠状动脉窦中血液流动速度较低,最大血液流动速度为 0.16 m/s.当 $\alpha =5^\circ$ 时,主动脉瓣置换存在倾斜,主动脉瓣开口向升主动脉的左冠状动脉一侧倾斜,导致跨瓣血液流动也向该侧 倾斜,血液流动冲击升主动脉壁. 当 $\alpha =10^\circ$ 和 $\alpha=15^\circ$ 时,跨瓣血液流动向升主动脉壁倾斜的程度增加,主动脉壁附近血流速度较大,导致对升主动脉壁的冲击较大. 同时,更多的血液流入左冠状动脉窦,当 $\alpha =5^\circ$,$\alpha =10^\circ$和 $\alpha =15^\circ$ 时,峰值期主动脉窦中最大血液流动速度分别为 0.68 m/s,0.94 m/s 和 0.79 m/s.倾斜角度改变跨瓣血液流动方向,但并未显著改变最大血流速度. 当 $\alpha =0^\circ$,$\alpha =5^\circ$, $\alpha=10^\circ$ 和 $\alpha=15^\circ$ 时,最大跨瓣血液流动速度分别为 1.56 m/s,1.57 m/s,1.55 m/s 和 1.54 m/s.
图6
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图6峰值期不同倾斜角度时主动脉根部速度分布云图
Fig. 6Velocity contours of the aortic root with different tilted angles at peak systolic
不同主动脉瓣倾斜角度下,主动脉根部中最大血液流动速度相近,但主动脉瓣倾斜改变跨瓣血液流动方向,使血液冲击升主动脉壁,损伤升主动脉壁面的内皮细胞.研究[21,40]表明,当内皮细胞受到损伤,胶原蛋白和组织因子就会暴露在流动的血液中,导致血小板活化、凝血酶生成,最终形成血栓. 因此,当 $\alpha =10^\circ$ 和 $\alpha=15^\circ$ 时,跨瓣血流向升主动脉左冠状动脉一侧倾斜,导致血流冲击升主动脉壁幅度增大,易形成血栓.
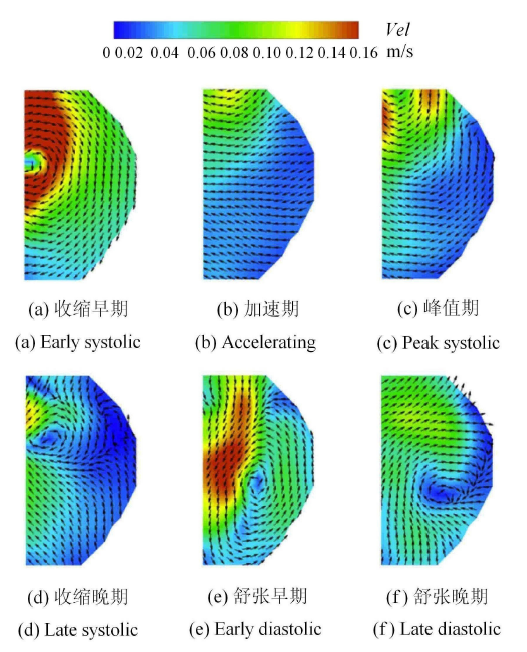
结合主动脉窦中血流速度分析实现对主动脉瓣附近流场的全面评估, $\alpha =0^\circ$ 时心动周期内主动脉窦的血液流动平均速度矢量和云图分布如图7 所示.收缩早期,主动脉瓣张开后,跨瓣流动的血液以 0.30 m/s 的速度进入主动脉窦并带动主动脉窦中静止的血液运动,形成涡旋,如图7(a) 所示.加速期,随着血液中心对称流动的发展,涡旋也向前运动发展,主动脉窦中最大血液流动速度降低至 0.12 m/s,如图7(b) 所示.峰值期,中心对称流动血液的速度较高,绝大部分血液充分向升主动脉流动,此时主动脉窦中仅存在较弱的涡旋运动,最大血液流动速度为 0.16 m/s,如图7(c) 所示.收缩晚期,跨瓣血液流动速度降低,部分升主动脉中的血液回流流向主动脉窦并形成涡旋,主动脉窦中最大血液流动速度为 0.14 m/s,如图7(d) 所示.舒张早期,主动脉窦中的涡旋以 0.17 m/s 的速度向瓣叶中部运动,促进瓣叶关闭,如图7(e) 所示.舒张晚期,主动脉窦中的涡旋向瓣叶基部运动,最大速度降低为 0.10 m/s,如图7(f) 所示.
图7
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图7$\alpha =0^\circ$ 时主动脉窦速度矢量和云图
Fig. 7Velocity vectors and contours of the aortic sinus at $\alpha =0^\circ$
不同倾斜角度时主动脉窦血液流动平均速度矢量和云图分布如图8 所示,在所有倾斜角度中存在明显的相同流动特征,即血液经过瓣叶后从主动脉窦的顶部流入主动脉窦,形成顺时针流动的涡旋. 当 $\alpha =5^\circ$ 和 $\alpha=10^\circ$ 时,收缩期时跨瓣血液在主动脉窦中部形成涡旋,并在整个收缩期向窦管交接处运动,该现象与文献[20] 趋势一致.在舒张期,当主动脉瓣逐渐关闭时,涡旋向主动脉窦底部运动. 随着倾斜角度增大至 $\alpha=15^\circ$ 时,主动脉瓣开口越向主动脉窦倾斜,导致更多的血液流动向主动脉窦倾斜,主动脉窦中的血液流动速度增大,涡旋更向主动脉窦底部运动.
图8
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图8不同倾斜角度时主动脉窦速度矢量和云图
Fig. 8Velocity vectors and contours of the aortic sinus with different tilted angles
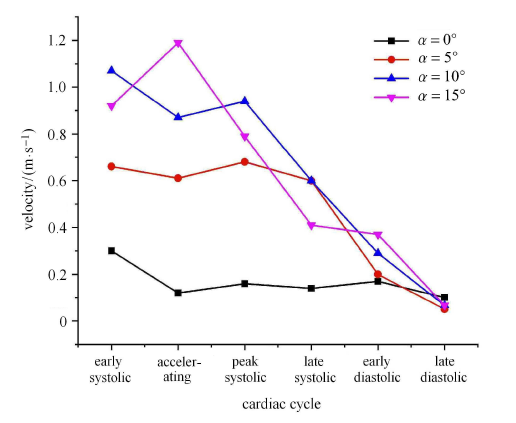
心动周期内不同倾斜角度时,主动脉窦的最大速度分布曲线如图9 所示. 值得注意的是,$\alpha=0^\circ$ 时心动周期内主动脉窦的血液流动速度较小 (如图6 所示),峰值期后主动脉窦中血液流动速度先增大后减小. 当 $\alpha=5^\circ$, $\alpha =10^\circ$ 和 $\alpha=15^\circ$ 时,即主动脉瓣置换存在倾斜时,心动周期内主动脉窦的血液流动速度较大,峰值期后主动脉窦中的血液流动速度持续减小.随着主动脉瓣置换倾斜角度增大,主动脉窦中的最大血液流动速度增大,当 $\alpha =0^\circ$,$\alpha =5^\circ$,$\alpha =10^\circ$ 和 $\alpha=15^\circ$ 时,心动周期内主动脉窦中最大血液流动速度分别为 0.30 m/s,0.68 m/s,1.07 m/s 和 1.19 m/s.
图9
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图9心动周期内不同倾斜角度时主动脉窦的最大速度分布曲线
Fig. 9Curves of peak velocity of the aortic sinus with different tilted angles during cardiac cycle
研究[41-42]表明,在收缩期,心肌收缩并限制血液向冠状动脉的流动,血流速度较低. 舒张期开始时,心肌肌肉松弛,导致冠状动脉血流速度迅速升高并达到峰值. 因此,当 $\alpha=0^\circ$ 时,主动脉窦中的血液流动速度先增大后减小,符合心动周期内血液由主动脉窦向冠状动脉流动的生理现象.当 $\alpha =5^\circ$, $\alpha =10^\circ$ 和 $\alpha=15^\circ$ 时,导致跨瓣血液流动的方向异常,改变了主动脉窦中血液流动状况,其最大血液流动速度随倾斜角度增大而增大,涡旋也更向主动脉窦底部运动,不利于血液从冠状动脉口流出向心肌供血.
2.2 倾斜角度对主动脉瓣下游涡度分布的影响
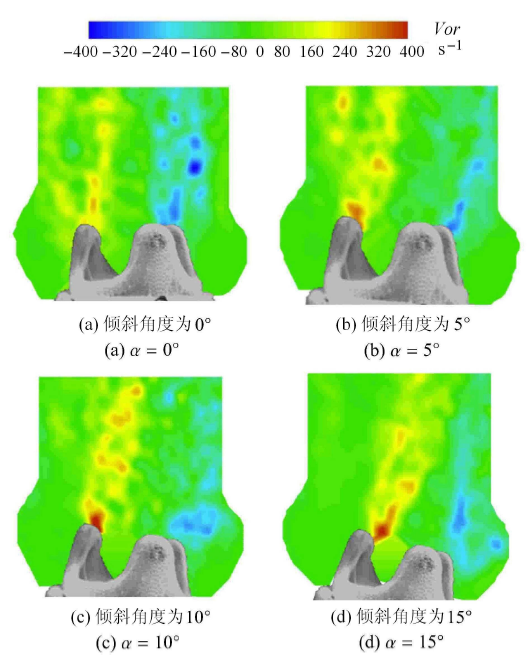
涡度是速度场的旋度,描述流体的旋转情况,高涡度区域表示流体中的高剪切区域[43],涡度由式 (1) 定义图10为峰值期不同倾斜角度下主动脉根部的涡度分布. 红色区域表示逆时针旋转 (正) 涡度,而蓝色区域表示顺时针旋转 (负) 涡度.不同倾斜角度时,涡度具有相似的分布情况,主动脉瓣血液流动边缘处存在较大的涡度区域.倾斜角度显著改变涡度分布情况,随着倾斜角度增大,高涡度区域向升主动脉壁倾斜. 当 $\alpha =0^\circ$, $\alpha=5^\circ$, $\alpha =10^\circ$ 和 $\alpha =15^\circ$ 时,正涡度分别为 270.30 s$^{ -1}$,371.18 s$^{ - 1}$, 502.24 s$^{ - 1}$ 和 412.35 s$^{ - 1}$,负涡度分别为 $-395.76$ s$^{- 1}$,$-321.32$ s$^{ - 1}$,$-274.17$ s$^{ - 1}$ 和 $-270.91$ s$^{ - 1}$.
图10
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图10峰值期不同倾斜角度时主动脉根部涡度分布云图
Fig. 10Vorticity contours of the aortic root with different tilted angles at peak systolic
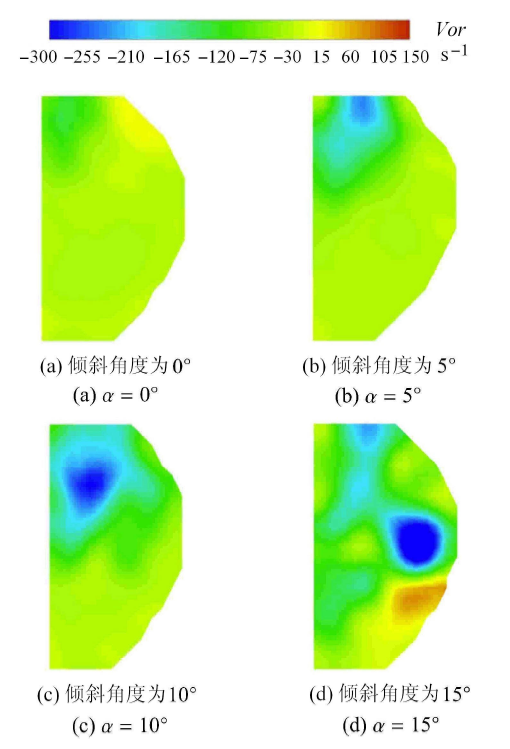
为评估主动脉瓣存在倾斜时对主动脉窦涡度分布影响,图11 展示了峰值期内不同倾斜角度下主动脉窦的涡度分布.$\alpha =0^\circ$ 时,主动脉窦中主要为较小的正涡度. $\alpha=5^\circ$ 时,主动脉窦中的负涡度增大,且负涡度位于瓣叶和窦管交接处中间.随着倾斜角度增大,负涡度逐渐增大,涡度逐渐位于主动脉窦底部,涡度方向和位置与图8 中涡旋运动一致.
图11
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图11峰值期不同倾斜角度时主动脉窦涡度分布云图
Fig. 11Vorticity contours of the aortic sinus with different tilted angles at peak systolic
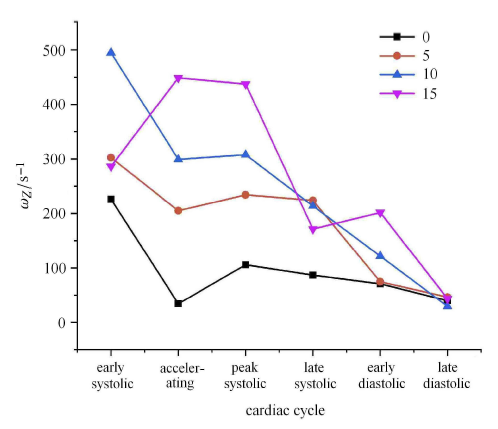
心动周期内不同倾斜角度时,主动脉窦的最大负涡度分布曲线如图12 所示. $\alpha=0^\circ$ 时,主动脉窦中负涡度较小,并呈 现先减小后增大再减小趋势. $\alpha =5^\circ$ 和 $\alpha=10^\circ$ 负涡度变化趋势与 $\alpha =0^\circ$ 时相同,但负涡度值增大. $\alpha=15^\circ$ 时,负涡度值变化在收缩期和舒张期均呈现先增大后减小趋势,负涡度值较大.随着倾斜角度的增大,峰值期主动脉窦中最大负涡度值增大. 当 $\alpha =0^\circ$,$\alpha =5^\circ$, $\alpha=10^\circ$ 和 $\alpha =15^\circ$ 时,心动周期内峰值期主动脉窦中最大负涡度分别为 $-105.64$ s$^{ -1}$,$-234.23$ s$^{ - 1}$,$-307.53$ s$^{ - 1}$ 和 $-437.19$ s$^{ - 1}$.
图12
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图12心动周期内不同倾斜角度时主动脉窦的最大负涡度分布曲线
Fig. 12Curves of peak negative vorticity of the aortic sinus with different tilted angles during cardiac cycle
研究[22]表明,涡度动力学在表征湍流中起着至关重要的作用,高涡度区域表示血液的剪切和旋转.Bark 等[23]的相 关研究也指出生理状态下主动脉的剪切率应低于 400 s$^{ -1}$,相当于黏性剪应力 1.4 N/m$^{2}$. 因此,倾斜角度 $\alpha =10^\circ$ 和 $\alpha=15^\circ$ 时主动脉根部和主动脉窦的剪切率水平较高,可能导致细胞溶血.
2.3 倾斜角度对主动脉瓣下游黏性剪应力分布的影响
黏性剪应力 (viscous shear stress, VSS) 表征流体相邻两层之间的剪切作用,是血细胞承受的真实物理剪应力,与瓣膜血栓、血小板及红细胞溶血密切相关[37,44-45],由式 (2) 定义峰值期,血液跨瓣流动后加速进入升主动脉,并且以心动周期内最大的射流速度与升主动脉中相对静止的血液相互剪切,形成剪切层.图13 为峰值期不同倾斜角度时主动脉根部黏性剪应力云图,由于最大速度梯度位于射流边缘,导致最大黏性剪应力值区域与射流边缘相对应,并且正、负黏性剪应力彼此相互平行. 当 $\alpha=0^\circ$ 时,主动脉瓣开口与升主动脉轴向平行,黏性剪应力与血液中心对称流动方向相同,即平行于升主动脉轴向.当 $\alpha=5^\circ$ 时,由于主动脉瓣倾斜,黏性剪应力随跨瓣血液流动方向朝着左冠状动脉窦一侧倾斜,几乎靠近升主动脉壁.当 $\alpha =10^\circ$ 时,负黏性剪应力完全与升主动脉壁平行. 当 $\alpha=15^\circ$ 时,随着主动脉瓣倾斜程度急剧增大,负黏性剪应力区域出现在主动脉窦.式中, $\mu $ 为工作流体的动力黏度,单位 N$\cdot $s/m$^{2}$.
图13
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图13峰值期不同倾斜角度时主动脉根部黏性剪应力云图
Fig. 13VSS contours of the aortic root with different tilted angles at peak systolic
主动脉瓣存在倾斜时,正黏性剪应力值较大、负黏性剪应力较小. $\alpha =0^\circ$,$\alpha =5^\circ$, $\alpha=10^\circ$ 和 $\alpha =15^\circ$ 时,正黏性剪应力值分别为 0.99 N/m$^{2}$,1.34 N/m$^{2}$,1.86 N/m$^{2}$ 和 1.37 N/m$^{2}$,负黏性剪应力值分别为 $-1.29$ N/m$^{2}$,$-0.96$ N/m$^{2}$,$-0.83$ N/m$^{2}$ 和 $-0.93$ N/m$^{2}$.Saw 等[46]研 究表明,大动脉血管的剪切应力值一般在 0.5 $\sim$ 2.0 N/m$^{2}$. Bark 等[23]的相关研究也指出生理状态下主动脉的黏性剪应力低于 1.4 N/m$^{2}$. 当主动脉瓣存在倾斜时,高黏性剪应力区域靠近升主动脉壁且出现在主动脉窦.$\alpha =10^\circ$ 和 $\alpha =15^\circ$时,最大黏性剪应力超过或接近临界剪应力阈值 1.4 N/m$^{2}$,容易发生红细胞溶血形成 血栓.
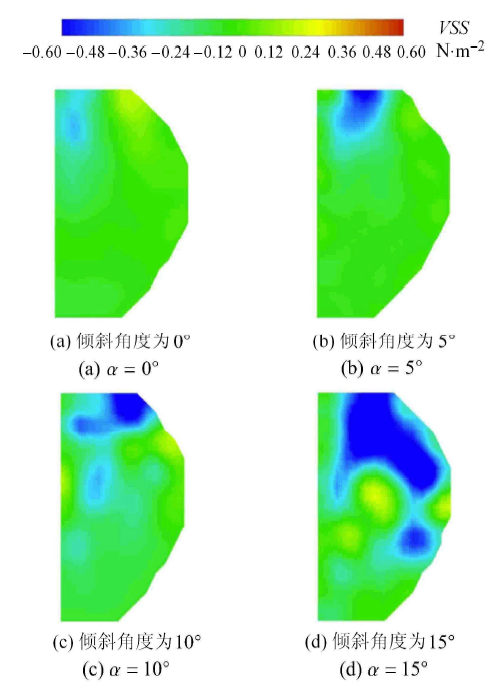
峰值期不同倾斜角度时主动脉窦黏性剪应力云图如图14 所示. 当 $\alpha =0^\circ$ 时,高黏性剪切区域位于主动脉窦中瓣叶一侧. 当 $\alpha =5^\circ$ 时,高黏性剪切应力区域位于窦管交接处,面积增大.随着倾斜程度增大,高黏性剪应力区域分布于主动脉窦壁面处,且面积持续增大.
图14
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图14峰值期不同倾斜角度时主动脉窦黏性剪应力云图
Fig. 14VSS contours of the aortic sinus with different tilted angles at peak systolic
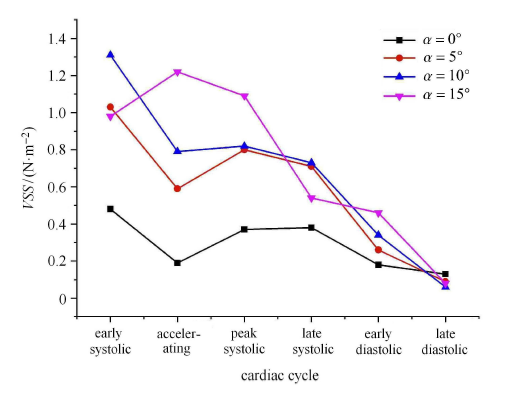
心动周期内不同倾斜角度时,主动脉窦的最大负黏性剪应力分布曲线如图15 所示. $\alpha=0^\circ$ 时,主动脉窦中负 黏性剪应力为先减小后增大再减小的变化趋势,且黏性剪应力值和变化范围较小. $\alpha=5^\circ$ 和 $\alpha =10^\circ$ 时,黏性剪应力曲线变化趋势与 $\alpha=0^\circ$ 时相似,但黏性剪应力值较大. 当 $\alpha=15^\circ$ 时,负黏性剪应力变化趋势先增大后减小,黏性剪应力值较大.随着倾斜角度的增大,峰值期主动脉窦中最大负黏性剪应力值增大. 当 $\alpha =0^\circ$,$\alpha =5^\circ$,$\alpha =10^\circ$ 和 $\alpha =15^\circ$ 时,心动周期内峰值期最大黏性剪应力值分别为 0.37 N/m$^{2}$,0.80 N/m$^{2}$,0.82 N/m$^{2}$ 和 1.09 N/m$^{2}$.
图15
 新窗口打开|下载原图ZIP|生成PPT
新窗口打开|下载原图ZIP|生成PPT图15心动周期内不同倾斜角度时主动脉窦的最大负黏性剪应力分布曲线
Fig. 15Curves of peak negative VSS of the aortic sinus with different tilted angles during cardiac cycle
主动脉窦血流动力学是影响主动脉瓣功能和健康的重要因素,异常的主动脉窦血流动力学将作用于主动脉瓣,引发主动脉瓣继发性疾病. 研究[47-48]表明,主动脉瓣钙化狭窄常发生在主动脉窦一侧的瓣叶处,主动脉瓣附近存在较高的黏性剪应力促进血栓形成.当主动脉瓣存在倾斜时,瓣叶附近黏性剪应力升高,为主动脉瓣发生病变提供了剪应力环境.
在主动脉瓣血流动力学研究中,血液流经瓣叶后在主动脉根部形成收缩射流,并在射流两侧边缘处产生较大的相反速度梯度值,形成正负黏性剪应力,其表征的是流体相邻两层之间瞬时剪切作用,与周围流体作用于血小板、血细胞的体积力相关,与细胞溶血、血栓形成等继发性瓣膜疾病密切相关,在血流动力学相关研究中广泛使用[49-50].
3 结论
本文研究了不同主动脉瓣倾斜角度下主动脉瓣下游的血流动力学,分析了倾斜角度对主动脉根部和主动脉窦的速度分布、涡度、黏性剪应力的影响,为临床主动脉瓣置换术提供流体力学参考. 研究结果对临床术前规划和术后康复具有重要意义. 主要结论如下.(1) 当 $\alpha =0^\circ$ 时,心动周期内跨瓣血液流动为中心对称流动,峰值期后主动脉窦中血液流动速度先增大后减小,涡旋运动促进瓣叶关闭. $\alpha =5^\circ$, $\alpha =10^\circ$ 和 $\alpha =15^\circ$ 时,跨瓣血液流动向升主动脉的左冠状动脉一侧倾斜,使血液冲击升主动脉壁,容易损伤升主动脉壁面的内皮细胞,导致血栓形成. 同时,主动脉瓣存在倾斜时也改变了主动脉窦中血液流动状况,最大血液流动速度随主动脉瓣倾斜角度增大而增大,涡旋也更向主动脉窦底部运动,不利于血液从冠状动脉口流出向心肌供血.
(2) 主动脉瓣置换角度存在倾斜时,由于血液跨瓣流动方向改变,主动脉根部的高涡度和黏性剪应力区域向升主动脉壁倾斜. 主动脉窦的高涡度区域位于主动脉窦底部、高黏性剪应力区域分布于主动脉窦壁面处.
(3) 主动脉瓣存在倾斜角度时,峰值期涡度和黏性剪应力较大. 特别是 $\alpha =10^\circ$ 和 $\alpha=15^\circ$ 时,主动 脉根部的最大涡度分别为 502.24 s$^{ - 1}$和412.35 s$^{ -1}$,最大黏性剪应力分别为 1.86 N/m$^{2}$ 和 1.37 N/m$^{2}$,为血栓形成提供了有利环境,临床主动脉瓣置换术时应规避.
参考文献 原文顺序
文献年度倒序
文中引用次数倒序
被引期刊影响因子
[本文引用: 1]
[本文引用: 1]
[本文引用: 1]
DOIURLPMID [本文引用: 1]
DOIURLPMID

Aortic valve replacement (AVR) does not usually restore physiological flow profiles. Complex flow profiles are associated with aorta dilatation, ventricle remodeling, aneurysms, and development of atherosclerosis. All these affect long-term morbidity and often require reoperations. In this pilot study, we aim to investigate an ability to optimize the real surgical AVR procedure toward flow profile associated with healthy persons. Four cases of surgical AVR (two with biological and two with mechanical valve prosthesis) with available post-treatment cardiac magnetic resonance imaging (MRI), including four-dimensional flow MRI and showing abnormal complex post-treatment hemodynamics, were investigated. All cases feature complex hemodynamic outcomes associated with valve-jet eccentricity and strong secondary flow characterized by helical flow and recirculation regions. A commercial computational fluid dynamics solver was used to simulate peak systolic hemodynamics of the real post-treatment outcome using patient-specific MRI measured boundary conditions. Then, an attempt to optimize hemodynamic outcome by modifying valve size and orientation as well as ascending aorta size reduction was made. Pressure drop, wall shear stress, secondary flow degree, helicity, maximal velocity, and turbulent kinetic energy were evaluated to characterize the AVR hemodynamic outcome. The proposed optimization strategy was successful in three of four cases investigated. Although no single parameter was identified as the sole predictor for a successful flow optimization, downsizing of the ascending aorta in combination with the valve orientation was the most effective optimization approach. Simulations promise to become an effective tool to predict hemodynamic outcome. The translation of these tools requires, however, studies with a larger cohort of patients followed by a prospective clinical validation study.
URLPMID [本文引用: 1]
DOIURL [本文引用: 1]
DOIURLPMID [本文引用: 1]
As the first section of a multi-part review series, this section provides an overview of the ongoing research and development aimed at fabricating novel heart valve replacements beyond what is currently available for patients. Here we discuss heart valve replacement options that involve a biological component or process for creation, either in vitro or in vivo (tissue-engineered heart valves), and heart valves that are fabricated from polymeric material that are considered permanent inert materials that may suffice for adults where growth is not required. Polymeric materials provide opportunities for cost-effective heart valves that can be more easily manufactured and can be easily integrated with artificial heart and ventricular assist device technologies. Tissue engineered heart valves show promise as a regenerative patient specific model that could be the future of all valve replacement. Because tissue-engineered heart valves depend on cells for their creation, understanding how cells sense and respond to chemical and physical stimuli in their microenvironment is critical and therefore, is also reviewed.
DOIURLPMID [本文引用: 1]
DOIURLPMID
DOIURLPMID
OBJECTIVES: The aim of this study was to assess the influence of amount and distribution of calcifications of the aortic valve and the left ventricular outflow tract on the acute procedural outcome of patients undergoing transcatheter aortic valve implantation (TAVI). BACKGROUND: Transcatheter aortic valve implantation is a new percutaneous technique especially for elderly, high-risk patients with significant aortic valve stenosis (AS). After TAVI, post-interventional paravalvular aortic regurgitations (PAR) can occur, which is believed to be related partially to valve calcifications. METHODS: We prospectively analyzed 100 symptomatic patients with severe AS scheduled for TAVI with the CoreValve ReValving (Medtronic, Minneapolis, Minnesota) prosthesis. In all patients, a native and contrast-enhanced multislice cardiac computed tomography was performed pre-interventionally. Calcification load of the valve and the adjacent outflow tract was estimated by the Agatston Score (AgS), and the amount and distribution of calcification was semi-quantitatively assessed and graded on a 1 to 4 scale (device
DOIURLPMID [本文引用: 2]
Prosthesis positioning in transcatheter aortic valve implantation procedures represents a crucial aspect for procedure success as demonstrated by many recent studies on this topic. Possible complications, device performance, and, consequently, also long-term durability are highly affected by the adopted prosthesis placement strategy. In the present work, we develop a computational finite element model able to predict device-specific and patient-specific replacement procedure outcomes, which may help medical operators to plan and choose the optimal implantation strategy. We focus in particular on the effects of prosthesis implantation depth and release angle. We start from a real clinical case undergoing Corevalve self-expanding device implantation. Our study confirms the crucial role of positioning in determining valve anchoring, replacement failure due to intra or para-valvular regurgitation, and post-operative device deformation.
DOIURLPMID [本文引用: 1]
BACKGROUND AND AIM OF THE STUDY: Aortic hemodynamics influence the integrity of the vessel wall and cardiac afterload. The aim of this study was to compare hemodynamics distal to biological (BV) and mechanical aortic valve (MV) replacements by in vitro 4D Flow MRI excluding confounding factors of in-vivo testing potentially influencing hemodynamics. METHODS: Two BV (Perimount MagnaEase [Carpentier-Edwards], Trifecta [Abbott]) and two MV (On-X [CryoLife], prototype trileaflet valve) were scanned in a flexible aortic phantom at 3T using a recommended 4D Flow MR sequence. A triphasic aortic flow profile with blood-mimicking fluid was established. Using GTFlow (Gyrotools), area and velocity of the ejection jet were measured. Presence and extent of sinus vortices and secondary flow patterns were graded on a 0 to 3 scale. RESULTS: A narrow, accelerated central ejection jet (Area = 27 +/- 7% of vessel area, Velocity = 166 +/- 13 cm/s; measured at sinotubular junction) was observed in BV as compared to MV (Area = 53 +/- 13%, Velocity = 109 +/- 21 cm/s). As opposed to MV, the jet distal to BV impacted the outer curvature of the ascending aorta and resulted in large secondary flow patterns (BV: n = 4, grades 3, 3, 2, 1; MV: n = 1, grade 1). Sinus vortices only formed distal to MV. Although physiologically configured, they were larger than normal (grade 3). CONCLUSIONS: In contrast to mechanical valves, biological valve replacements induced accelerated and increased flow patterns deviating from physiological ones. While it remains speculative whether this increases the risk of aneurysm formation through wall shear stress changes, findings are contrasted by almost no secondary flow patterns and typical, near-physiological sinus vortex formation distal to mechanical valves.
DOIURLPMID [本文引用: 1]
Aortic stenosis caused by valve calcification is a major cause of death around the world. Hemodynamic factors have been suggested to be major players in the development of valve calcification, yet a detailed knowledge of the blood flow dynamics as experienced by endothelial cells on valve surfaces is still lacking. In this study we carry out high-resolution numerical simulations of the blood flow through a polymeric trileaflet valve in order to elucidate the differential flow dynamics on the aortic and ventricular sides of the valve leaflets. Limiting streamlines and surface shear stress contours are used to probe and quantify the blood flows on its side. Complicated flow patterns were only observed on the aortic side of the valve near the region where focalized distribution of valve calcification is typically observed.
[本文引用: 2]
DOIURLPMID
Transcatheter aortic valve implantation is a novel treatment for severe aortic valve stenosis. Due to the recent use of this technology and the procedural variability, there is very little data that quantify the hemodynamic consequences of variations in valve placement. Changes in aortic wall stresses and fluid retention in the sinuses of Valsalva can have a significant effect on the clinical response a patient has to the procedure. By comprehensively characterizing complex flow in the sinuses of Valsalva using digital particle image velocimetry and an advanced heart-flow simulator, various positions of a deployed transcatheter valve with respect to a bioprosthetic aortic valve (valve-in-valve) were tested in vitro. Displacements of the transcatheter valve were axial and directed below the simulated native valve annulus. It was determined that for both blood residence time and aortic Reynolds stresses, it is optimal to have the annulus of the transcatheter valve deployed as close to the aortic valve annulus as possible.
DOIURLPMID [本文引用: 2]
PURPOSE: The physiological flow dynamics within the Valsalva sinuses, in terms of global and local parameters, are still not fully understood. This study attempts to identify the physiological conditions as closely as possible, and to give an explanation of the different and sometime contradictory results in literature. METHODS: An in vitro approach was implemented for testing porcine bio-prosthetic valves operating within different aortic root configurations. All tests were performed on a pulse duplicator, under physiological pressure and flow conditions. The fluid dynamics established in the various cases were analysed by means of 2D Particle Image Velocimetry, and related with the achieved hydrodynamic performance. RESULTS: Each configuration is associated with substantially different flow dynamics, which significantly affects the valve performance. The configuration most closely replicating healthy native anatomy was characterised by the best hemodynamic performance, and any mismatch in size and position between the valve and the root produced substantial modification of the fluid dynamics downstream of the valve, hindering the hydrodynamic performance of the system. The worst conditions were observed for a configuration characterised by the total absence of the Valsalva sinuses. CONCLUSION: This study provides an explanation for the different vortical structures described in the literature downstream of bioprosthetic valves, enlightening the experimental complications in valve testing. Most importantly, the results clearly identify the fluid mechanisms promoted by the Valsalva sinuses to enhance the ejection and closing phases, and this study exposes the importance of an optimal integration of the valve and root, to operate as a single system.
DOIURLPMID [本文引用: 1]
/= 50, the likelihood of occurrence of significant AR could be predicted with a sensitivity of 85% and a specificity of 87%. CONCLUSIONS: The occurrence of significant AR after TAVI can be predicted by anatomic and procedural variables. A model such as that presented can be used to select suitable patients for this procedure and guide operators during implantation of the device.]]>
URLPMID [本文引用: 3]
DOIURLPMID [本文引用: 1]
Restenosis and thrombosis are potentially fatal complications of coronary stenting with a recognized multifactorial etiology. The effect of documented risk factors, however, cannot explain the preponderance of certain lesion types, stent designs, and implantation configurations for the development of these complications. Local hemodynamic factors, low endothelial shear stress (ESS) in particular, are long known to critically affect the natural history of atherosclerosis. Increasing evidence now suggests that ESS may also contribute to the development of restenosis and thrombosis upon stenting of atherosclerotic plaques, in conjunction with well-appreciated risk factors. In this review, we present in vivo and mechanistic evidence associating ESS with the localization and progression of neointimal hyperplasia and in-stent clotting. Clinical studies have associated stent design features with the risk of restenosis. Importantly, computational simulations extend these observations by directly linking specific stent geometry and positioning characteristics with the post-stenting hemodynamic milieu and with the stent's thrombogenicity and pro-restenotic potential, thereby indicating ways to clinical translation. An enhanced understanding of the pathophysiologic role of ESS in restenosis and thrombosis might dictate hemodynamically favorable stent designs and deployment configurations to reduce the potential for late lumen loss and thrombotic obstruction. Recent methodologies for in vivo ESS profiling at a clinical level might allow for early identification of patients at high risk for the development of restenosis or thrombosis and might thereby guide individualized, risk-tailored treatment strategies to prevent devastating complications of endovascular interventions.
[本文引用: 1]
DOIURLPMID [本文引用: 3]
6,000 s(-1) (P
[本文引用: 1]
[本文引用: 1]
[本文引用: 1]
DOIURLPMID
Flow fields in the distal end-to-side anastomosis of coronary artery bypass graft are associated with intimal hyperplasia and bypass failure. This work aims to demonstrate the effect of anastomotic angle and diameter ratio on flow field of coronary artery bypass graft. The flow fields inside polydimethylsiloxane models of coronary artery bypass graft with various anastomotic angles (alpha = 30 degrees , 45 degrees , 60 degrees and 75 degrees ) and different diameter ratios (Phi = 0.78 and 1.11) are investigated using particle image velocimetry and computational fluid dynamics method under pulsatile flow condition. The results show that the anastomotic angle is positively correlated with the number and area of the recirculation zone, and the flow field disturbance at the anastomosis will develop in the same direction. Compared with that of Phi = 0.78, when Phi = 1.11, the flow fields at the anastomosis are relatively smoother with less turbulence.
[本文引用: 1]
DOIURLPMID [本文引用: 1]
[本文引用: 1]
[本文引用: 1]
[本文引用: 1]
[本文引用: 1]
DOIURLPMID [本文引用: 1]
[本文引用: 2]
URLPMID [本文引用: 1]
URLPMID [本文引用: 1]
DOIURLPMID [本文引用: 1]
INTRODUCTION: Blood flow induced shear stress plays an important role in platelet and endothelial cell functions. The goal of this study was to investigate the effect of physiologically relevant dynamic shear stress on platelet and endothelial cells. MATERIALS AND METHODS: Pulsatile shear stress waveforms mimicking the flow in a normal left coronary artery (0.1-1 Pa), at a 60% stenosis (0.2 - 6 Pa) and in the recirculation zone (0.01 - 0.5 Pa) behind a stenosis were used to stimulate platelets and endothelial cells in a cone and plate shearing device. Platelet activation was measured by CD62P expression and thrombogenicity. Meanwhile, endothelial cell activation and damage was measured by cell surface ICAM-1 and tissue factor expression using fluorescence microscopy. Endothelial tissue factor activity was measured using a commercial kit. RESULTS: Results showed that for platelets, a short exposure to elevated shear stress at the stenosis throat did not induce significant increase in platelet activation or thrombogenicity. While the low pulsatile shear stress had a potential for enhanced thrombosis. Both low and high pulsatile shear stress led to a significant increase in ICAM-1 expression on endothelial cell surface, but only low shear stress caused tissue factor over expression and enhanced tissue factor activity. CONCLUSION: These results suggest that low pulsatile shear stress may be more atherogenic, compared to elevated shear stress induced by stenosis.
DOIURLPMID [本文引用: 1]
Impairment of coronary artery flow, in either acute or chronic conditions, is a severe complication of transcatheter aortic valve (TAV) implantation, which can arise due to improper TAV positioning. However, little work has been done to quantify the effects of the TAV positioning on the coronary flow. In this study, a realistic in vitro model of coronary artery flow was developed and used to investigate the impact of TAV deployed orientations on coronary flow. The coronary hemodynamics was first replicated mathematically using a lumped parameter model with time-varying myocardial resistance. Based on the analytical model, two stepper motor controlled stopcock valves were integrated in a left heart simulator to represent the variable myocardial resistance in the experimental setup. The coronary flow and pressure waveforms obtained from the in vitro system were consistent with published data. With a TAV deployed in different orientations, the measured results demonstrated that TAV orientation does not have a significant impact on the coronary flow. The developed in vitro model can be further utilized to simulate coronary flow under various pathological conditions.
[本文引用: 1]
DOIURLPMID [本文引用: 1]
URLPMID [本文引用: 1]
DOIURL [本文引用: 1]
URLPMID [本文引用: 1]
DOIURLPMID [本文引用: 1]
The regulation of valvular endothelial phenotypes by the hemodynamic environments of the human aortic valve is poorly understood. The nodular lesions of calcific aortic stenosis (CAS) develop predominantly beneath the aortic surface of the valve leaflets in the valvular fibrosa layer. However, the mechanisms of this regional localization remain poorly characterized. In this study, we combine numerical simulation with in vitro experimentation to investigate the hypothesis that the previously documented differences between valve endothelial phenotypes are linked to distinct hemodynamic environments characteristic of these individual anatomical locations. A finite-element model of the aortic valve was created, describing the dynamic motion of the valve cusps and blood in the valve throughout the cardiac cycle. A fluid mesh with high resolution on the fluid boundary was used to allow accurate computation of the wall shear stresses. This model was used to compute two distinct shear stress waveforms, one for the ventricular surface and one for the aortic surface. These waveforms were then applied experimentally to cultured human endothelial cells and the expression of several pathophysiological relevant genes was assessed. Compared to endothelial cells subjected to shear stress waveforms representative of the aortic face, the endothelial cells subjected to the ventricular waveform showed significantly increased expression of the
DOIURLPMID [本文引用: 1]
OBJECTIVE: Valve-in-valve procedures using transcatheter aortic valves are increasingly performed to treat degenerated bioprosthetic surgical aortic valves because they are less invasive than redo aortic valve replacement. The objective of this study is to quantify the changes in aortic sinus blood flow dynamics before and after a valve-in-valve procedure to gain insight into mechanisms for clinical and subclinical thrombosis of leaflets. METHODS: A detailed description of the sinus hemodynamics for valve-in-valve implantation was performed in vitro. A Medtronic Hancock II (Medtronic Inc, Minneapolis, Minn) porcine bioprosthesis was modeled as a surgical aortic valve, and Medtronic CoreValve and Edwards Sapien (Edwards Lifesciences, Irvine, Calif) valves were used as the transcatheter aortic valves. High-resolution particle image velocimetry was used to compare the flow patterns from these 2 valves within both the left coronary and noncoronary sinuses in vitro. RESULTS: Velocity and vorticity within the surgical valve sinuses reached peak values of 0.7 m/s and 1000 s(-1), with a 70% decrease in peak fluid shear stress near the aortic side of the leaflet in the noncoronary sinus. With the introduction of transcatheter aortic valves, peak velocity and vorticity were reduced to approximately 0.4 m/s and 550 s(-1) and 0.58 m/s and 653 s(-1) without coronary flow and 0.60 m/s and 631 s(-1) and 0.81 m/s and 669 s(-1) with coronary flow for the CoreValve and Sapien valve-in-valve implantations, respectively. Peak shear stress was approximately 38% higher along the aortic side of the coronary versus noncoronary transcatheter aortic valve leaflet. CONCLUSIONS: Decreased flow and shear stress in valve-in-valve procedures indicate a higher risk of leaflet thrombosis secondary to flow stasis, perhaps more so in the noncoronary sinus.
DOIURLPMID [本文引用: 1]
The bicuspid aortic valve (BAV) is a common congenital malformation of the aortic valve (AV) affecting 1% to 2% of the population. The BAV is predisposed to early degenerative calcification of valve leaflets, and BAV patients constitute 50% of AV stenosis patients. Although evidence shows that genetic defects can play a role in calcification of the BAV leaflets, we hypothesize that drastic changes in the mechanical environment of the BAV elicit pathological responses from the valve and might be concurrently responsible for early calcification. An in vitro model of the BAV was constructed by surgically manipulating a native trileaflet porcine AV. The BAV valve model and a trileaflet AV (TAV) model were tested in an in vitro pulsatile flow loop mimicking physiological hemodynamics. Laser Doppler velocimetry was used to make measurements of fluid shear stresses on the leaflet of the valve models using previously established methodologies. Furthermore, particle image velocimetry was used to visualize the flow fields downstream of the valves and in the sinuses. In the BAV model, flow near the leaflets and fluid shear stresses on the leaflets were much more unsteady than for the TAV model, most likely due to the moderate stenosis in the BAV and the skewed forward flow jet that collided with the aorta wall. This additional unsteadiness occurred during mid- to late-systole and was composed of cycle-to-cycle magnitude variability as well as high-frequency fluctuations about the mean shear stress. It has been demonstrated that the BAV geometry can lead to unsteady shear stresses under physiological flow and pressure conditions. Such altered shear stresses could play a role in accelerated calcification in BAVs.
DOIURLPMID [本文引用: 1]
Patients with aortic stenosis present with calcium deposits on the native aortic valve, which can result in non-concentric expansion of Transcatheter Aortic Valve Replacement (TAVR) stents. The objective of this study is to evaluate whether eccentric deployment of TAVRs lead to turbulent blood flow and blood cell damage. Particle Image Velocimetry was used to quantitatively characterize fluid velocity fields, shear stress and turbulent kinetic energy downstream of TAVRs deployed in circular and eccentric orifices representative of deployed TAVRs in vivo. Effective orifice area (EOA) and mean transvalvular pressure gradient (TVG) values did not differ substantially in circular and eccentric deployed valves, with only a minor decrease in EOA observed in the eccentric valve (2.0 cm(2) for circular, 1.9 cm(2) for eccentric). Eccentric deployed TAVR lead to asymmetric systolic jet formation, with increased shear stresses (circular = 97 N/m(2) vs. eccentric = 119 N/m(2)) and regions of turbulence intensity (circular = 180 N/m(2) vs. eccentric = 230 N/m(2)) downstream that was not present in the circular deployed TAVR. The results of this study indicate that eccentric deployment of TAVRs can lead to altered flow characteristics and may potentially increase the hemolytic potential of the valve, which were not captured through hemodynamic evaluation alone.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}